The Technique for the Carolina Bridge
The Carolina bridge is an all-porcelain bonded pontic that can be used as an interim prosthesis and for many other valuable purposes.
In my last blog, I discussed why I love the Carolina bridge and its many applications as a restorative alternative. Now, I’ll provide an overview of the design and how to begin a case using the bridge.
Carolina Bridge Design
The design of the Carolina bridge bypasses problems found in Maryland bridges and adhesion bridges. The all-porcelain Carolina bridge is very esthetic because there is no metal substructure. There is also incredible light penetration.
Maryland bridges, on the other hand, are not esthetic due to the the graying created by metal wings. All-porcelain pontics, such as the Carolina bridge, often can be used when tooth anatomy comes before or restricts the prep and placement of a Maryland-type bridge. Also, it is easier to repair the proximal resin composite retaining connectors of Carolina bridges.
Carolina Bridge Case Technique
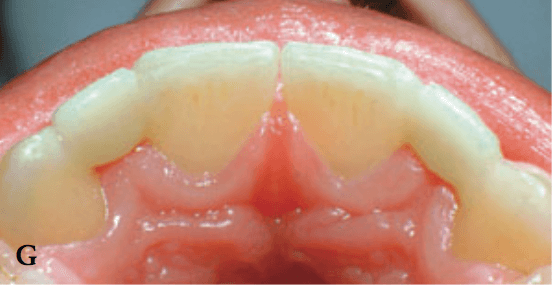
A case that illustrates a Carolina bridge technique is one where an adolescent patient presented with a missing maxillary right lateral incisor. A team consisting of a periodontist, an orthodontist, an endodontist, and a restorative dentist determined that a dental implant would be the best treatment once the patient reaches maturity.
The team decided to orthodontically submerge the endodontically treated root to best preserve the bony site for implant placement. They selected a Carolina bridge as the best interim prosthesis because the occlusal relationship was favorable and there was sufficient crown length of the abutment teeth.
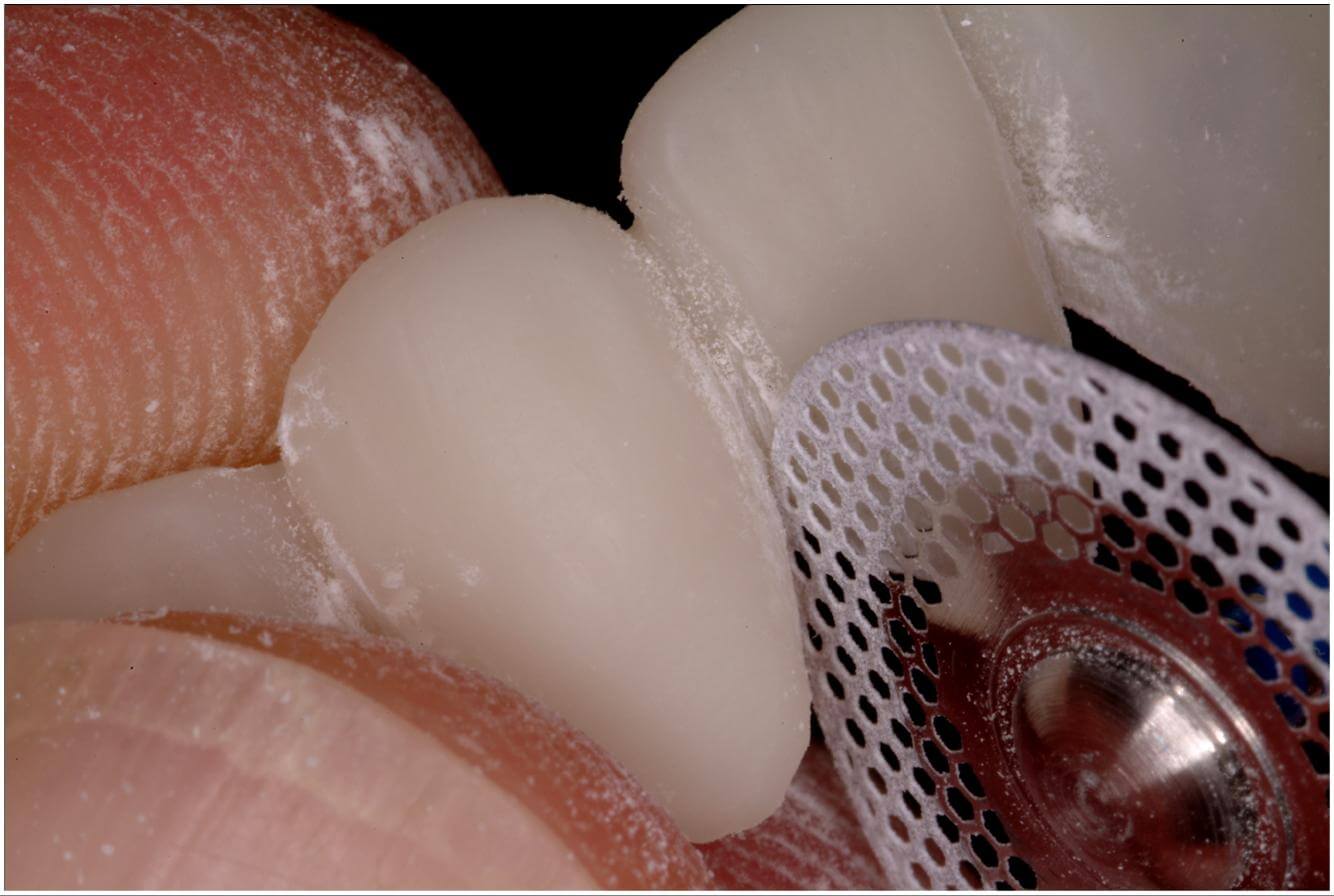
At the first appointment, shade selection was determined and an elastomeric impression was made of the anterior segment. A working case, an impression of the opposing arch, and a bite registration were created. An all-porcelain pontic was fabricated of feldspathic porcelain by the laboratory. At the second appointment, the involved abutment teeth were fully cleaned and rinsed.
The pontic was trial positioned to assess the shade accuracy and the adaptation of the pontic to the residual ridge. Once the accuracy of the shade and fit was verified, the pontic was readied for cementation.
A silane coupling agent was placed on the etched proximal surfaces of the porcelain pontic to improve the bond strength. Preparation of the abutment teeth was done by lightly roughening the proximal surfaces with a coarse, flame-shaped diamond stone. At this point, the pontic was ready for bonding into the edentulous space.
Dr. Heymann will be a featured lecturer at the Pankey 2018 Annual Meeting in Nashville, TN.





Related Course

Worn Dentition: Direct & Indirect Adhesive Management Through a Non-Invasive Approach
DATE: October 24 2025 @ 8:00 am - October 25 2025 @ 2:30 pmLocation: The Pankey Institute
CE HOURS: 15
Dentist Tuition : $ 2595
Single Occupancy with Ensuite Private Bath (per night): $ 345
Enhance Restorative Outcomes The main goal of this course is to provide, indications and protocols to diagnose and treat severe worn dentition through a new no prep approach increasing the…
Learn More>
About Author
Dr. Heymann is particularly active in the clinical research of esthetic restorative materials and participates in a dental practice devoted largely to esthetic dentistry. He is a member of the Academy of Operative Dentistry, the International Association of Dental Research, and is past-president and a fellow of the American Academy of Esthetic Dentistry. He is also a fellow in the International College of Dentists, the American College of Dentists, and the Academy of Dental Materials. He also serves as a consultant to the ADA. The author of more than 190 scientific publications, Dr. Heymann is co-senior editor of Sturdevant's Art and Science of Operative Dentistry and the editor-in-chief of the Journal of Esthetic and Restorative Dentistry. He has given more than 1,400 lectures on various aspects of esthetic dentistry worldwide and has received the Gordon J. Christensen Award for excellence as a CE speaker. Dr. Heymann graduated from the University of North Carolina School of Dentistry. He is past chair and graduate program director of the department of operative dentistry and currently is the Thomas P. Hinman Distinguished Professor of Operative Dentistry at the UNC School of Dentistry