Caring for a Dental Leaf Gauge
Caring for a Dental Leaf Gauge
Lee Ann Brady, DMD
In the Pankey Essentials courses, we use dental leaf gauges to train dentists in how to feel for the first point of occlusal contact, as a method for occlusal deprogramming, and as a tool for articulating models on an articulator in centric relation. Dental leaf gauges not only assist us in diagnosis and treatment planning but also in enabling our patients to discover the nature of their occlusion as we help them understand how malocclusion can manifest in TMD symptoms, parafunction, tooth damage, and more.
In our Essentials 1 course, I am sometimes asked how to take care of leaf gauges, so I thought I would share my answer.
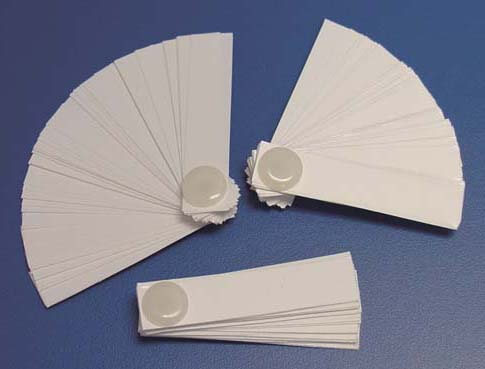
Although they don’t last forever, dental leaf gauges do last a long time and you can autoclave them between uses. When you sterilize them, the leaves become sticky, so I separate them like a hand of cards before putting the gauge in the autoclave bag and separate them again when I take them out of the bag just before going to the mouth.
Over time, with use, a leaf gauge will start to look a little beat up. I’m looking at one now. The Teflon screw that holds it together has turned color from going through the autoclave. I can see some ink stains from Madame Butterfly silk. It’s at the point where I think it looks too grungy to keep using. Although it might continue functioning for quite some time, I’m going to toss it and use a new one. After all, they are relatively low cost with a high return on investment.
I’ve never seen a dental leaf gauge break after many trips through the autoclave. I tested cold sterilizing one and discovered the chemistry in the ultrasonic cleaner started to make the leaves brittle and they came out stickier than when autoclaved. So, my preference (and the protocol in my practice) is to bag them and put them through the autoclave.





Related Course

TMD & Orofacial Pain: Managing Complex Patients
DATE: January 29 2025 @ 8:00 am - February 2 2025 @ 1:00 pmLocation: The Pankey Institute
CE HOURS: 37
Dentist Tuition: $ 7200
Single Occupancy with Ensuite Private Bath (per night): $ 345
THIS COURSE IS SOLD OUT TMD patients present with a wide range of concerns and symptoms from tension headaches and muscle challenges to significant joint inflammation and breakdown. Accurate thorough…
Learn More>Related Article

About Author


