QuickSplint for Diagnostics and Restorative Applications
QuickSplint has many functions in general practice, but it is also a great resource overall in both diagnostics and restorative dentistry. It’s ideal for patients who grind, those with endodontic issues, and anyone needing a restoration.
QuickSplint to Improve the Patient Experience
Many dentists see patients who have wear on their teeth but don’t think they grind at all. They might have said that they used to grind their teeth, but they believe they don’t anymore. You can use the QuickSplint as a learning experience where the patient is able to recognize the cause of the attrition.
It’s nice to rely on this quick, easy, and inexpensive device. Go ahead and have the patient sleep in it for a little while. The QuickSplint will then reveal whether or not they are clenching and grinding. After the proof is clearly demonstrated, you can have an impactful conversation with your patient.
Another option for QuickSplint use is as a means for handling parafunction and restorative materials selection. Today, we talk a lot about posterior materials when we are doing crowns on first or second molars. Are we going to use high strength ceramics or traditional PFM restorations? Instead of guessing about the patient’s parafunctional risk and how much load they will place on the restoration, you can easily get that information with a QuickSplint.
Additionally, you can use the QuickSplint as a post-op device after an endodontic procedure. You can reduce a patient’s discomfort significantly in less than three minutes and also help the tooth heal without occlusal pressure. You then won’t have to take the entire occlusal table off the problem tooth. This can even work during pre-op for a patient whose tooth appears to need endodontic treatment.
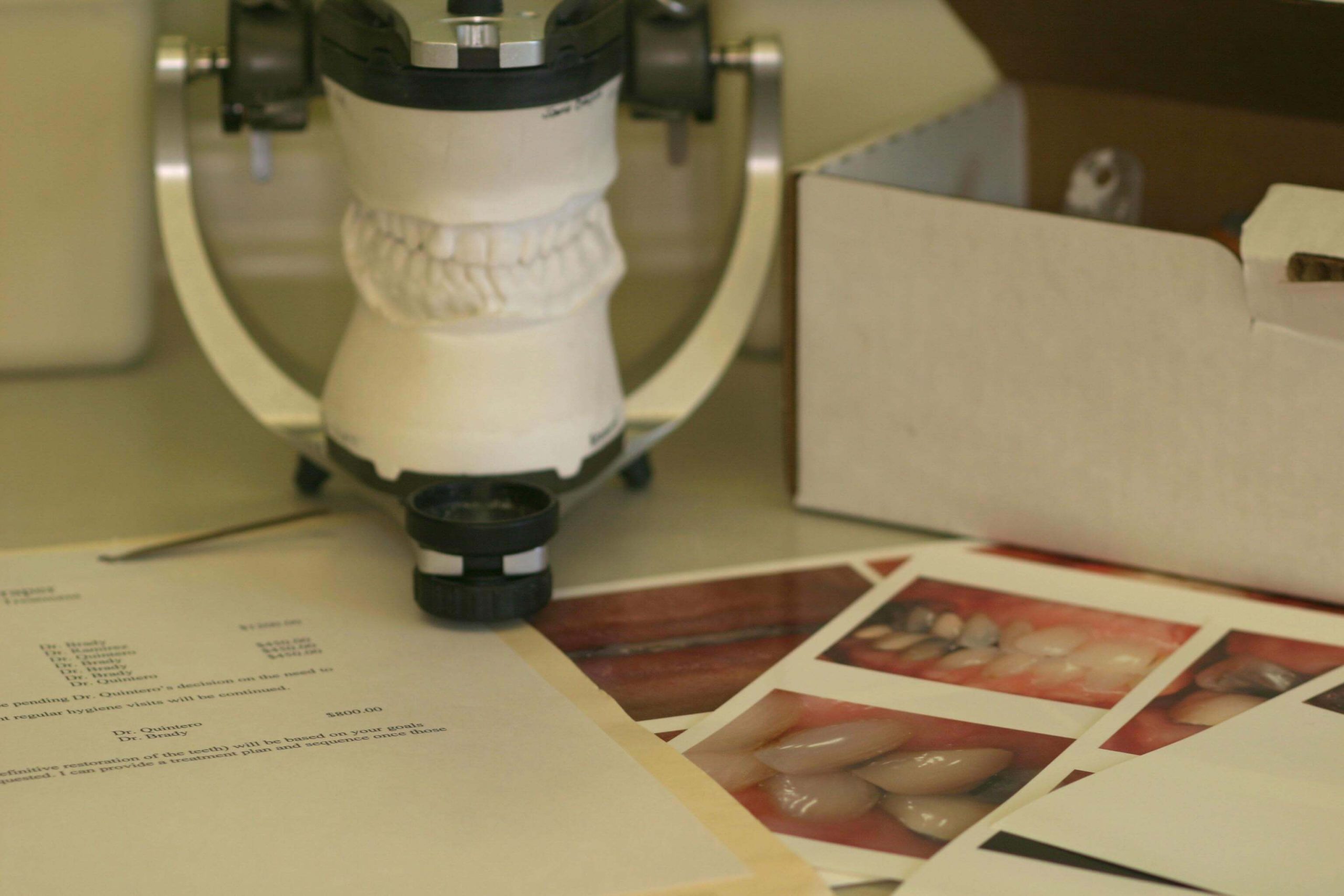
In our Essentials One course at Pankey we use the Quicksplint as an overnight deprogrammer to allow us to capture very accurate diagnostic records.
Do you use QuickSplint in your dental practice? Tell us your best tips for using this handy little tool!





Related Course

E3: Restorative Integration of Form & Function
DATE: March 30 2025 @ 8:00 am - April 3 2025 @ 2:30 pmLocation: The Pankey Institute
CE HOURS: 41
Dentist Tuition: $ 7400
Single Occupancy with Ensuite Private Bath (per night): $ 345
Understanding that “form follows function” is critical for knowing how to blend what looks good with what predictably functions well. E3 is the phase of your Essentials journey in which…
Learn More>
About Author