Dento-Facial Analyzer Technique: Capturing Records
You can gather accurate functional and esthetic information using the Panadent Dento-Facial Analyzer for restorative cases. I’ve found this tool particularly effective compared to alternatives such as the Facebow or stick bite.
If you haven’t done so yet, make sure to check out the introduction to this series on the Dento-Facial Analyzer. It includes background information, armamentarium, and key reasons why the device can elevate patient care.
Without further ado, the Dento-Facial Analyzer technique:
Essentials of Dento-Facial Analyzer Technique
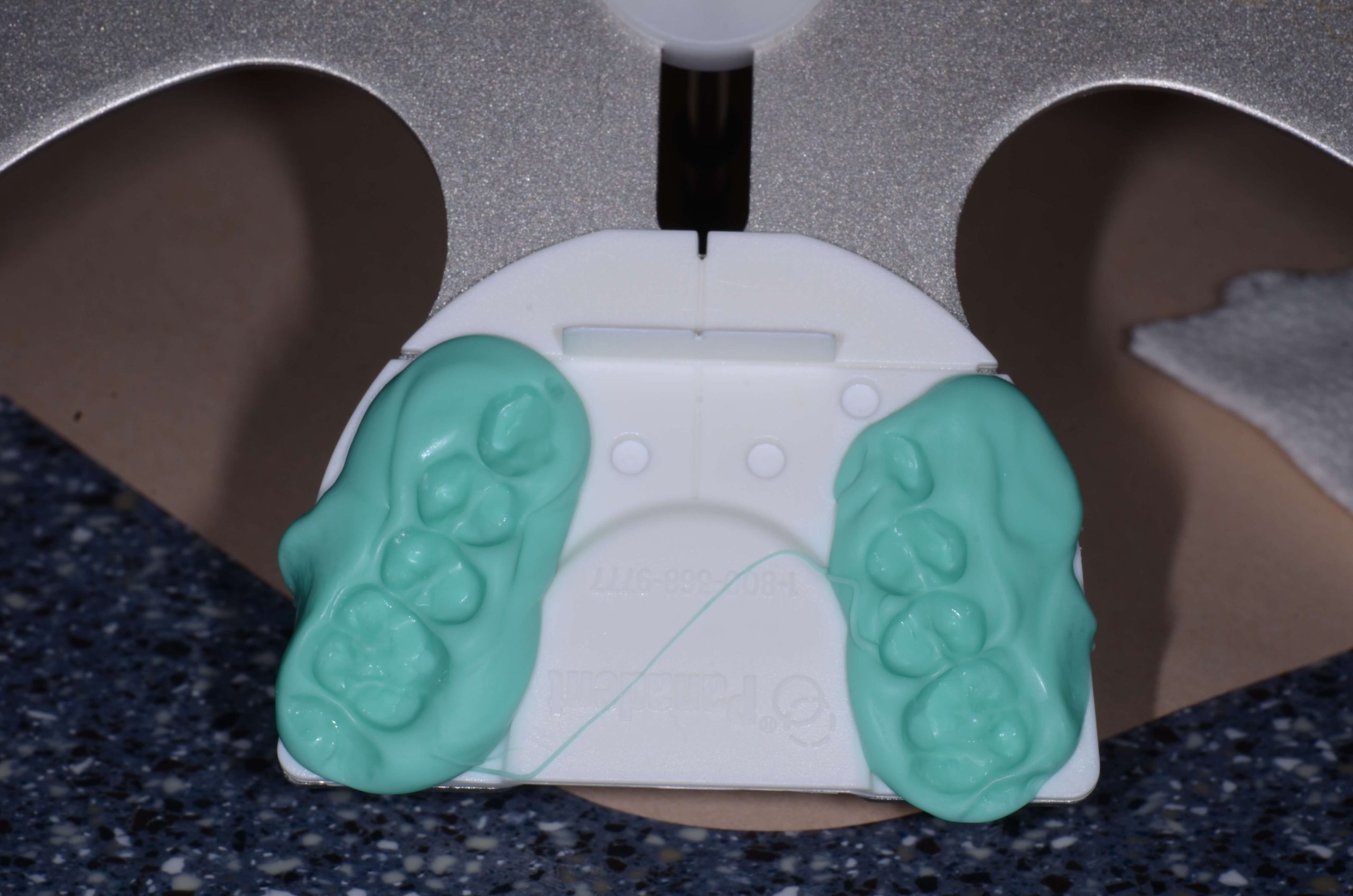
Once you have the white disposable plate – which is actually the piece you will send to the lab once the record is captured – snapped onto the Dento-Facial Analyzer, use VPS tray adhesive to lightly coat the plastic tray. You are only going to do this from about the canine position posteriorly because you aren’t going to put silicone on the anterior portion of that bite plate.
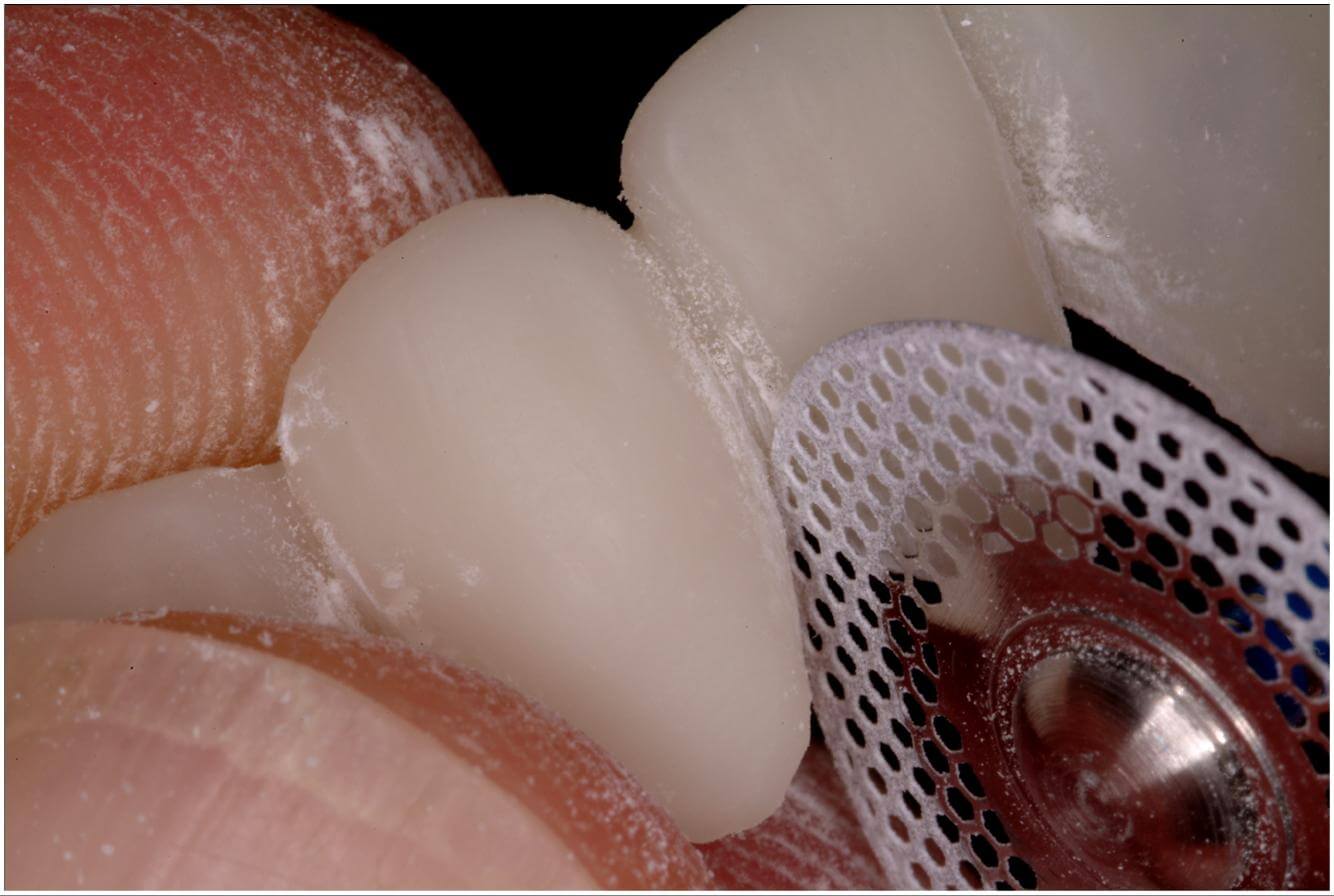
Next, attach the vertical reference bar to the Dento-Facial Analyzer. Without bite registration on it, take it to the patient’s mouth and seat the central incisors exactly against the white plastic in the front labially.
Verify that you can hold this level to the horizon in two planes of space and that you can touch the patient’s teeth. If not, you might need to build up the posterior.
If you’ve verified this, put bite silicone on the plate from the canine position back, then seat it again, making sure the central incisors are seated labially against the white plastic …
–
I’ll round up this fun technique with Part 3 in the series coming soon.
For a hands-on lesson in the Dento-Facial Analyzer from our talented educators, check out our Essentials 1 Pankey course. Also, watch this video for a quick refresher or pre-course overview.





Related Course

E2: Occlusal Appliances & Equilibration
DATE: July 21 2024 @ 8:00 am - July 25 2024 @ 2:30 pmWhat if you had one tool that increased comprehensive case acceptance, managed patients with moderate to high functional risk, verified centric relation and treated signs and symptoms of TMD? Appliance…
Learn More>
About Author
Dr. Lee Ann Brady is passionate about dentistry, her family and making a difference. She is a general dentist and owns a practice in Glendale, AZ limited to restorative dentistry. Lee’s passion for dental education began as a CE junkie herself, pursuing lots of advanced continuing education focused on Restorative and Occlusion. In 2005, she became a full time resident faculty member for The Pankey Institute, and was promoted to Clinical Director in 2006. Lee joined Spear Education as Executive VP of Education in the fall of 2008 to teach and coordinate the educational curriculum. In June of 2011, she left Spear Education, founded leeannbrady.com and joined the dental practice she now owns as an associate. Today, she teaches at dental meetings and study clubs both nationally and internationally, continues to write for dental journals and her website, sits on the editorial board of the Journal of Cosmetic Dentistry, Inside Dentistry and DentalTown Magazines and is the Director of Education for The Pankey Institute.