Restorative Tips: Successful Intracrevicular Tooth Preparation
Maintaining the gingival margin during a restoration is one of the more challenging aspects of restorative care. Part of why this can be so difficult is that the gingival crevice is not always well understood.
The goal with a restoration should be to limit the possibility of inflammation or gingivitis post-treatment. This can only be accomplished if the intracrevicular margins (meaning those placed within and limited to the gingival crevice) are properly created.
There are multiple techniques needed for this goal, but one critical piece is how the tooth is prepared.
Successful Tooth Preparation Guidelines
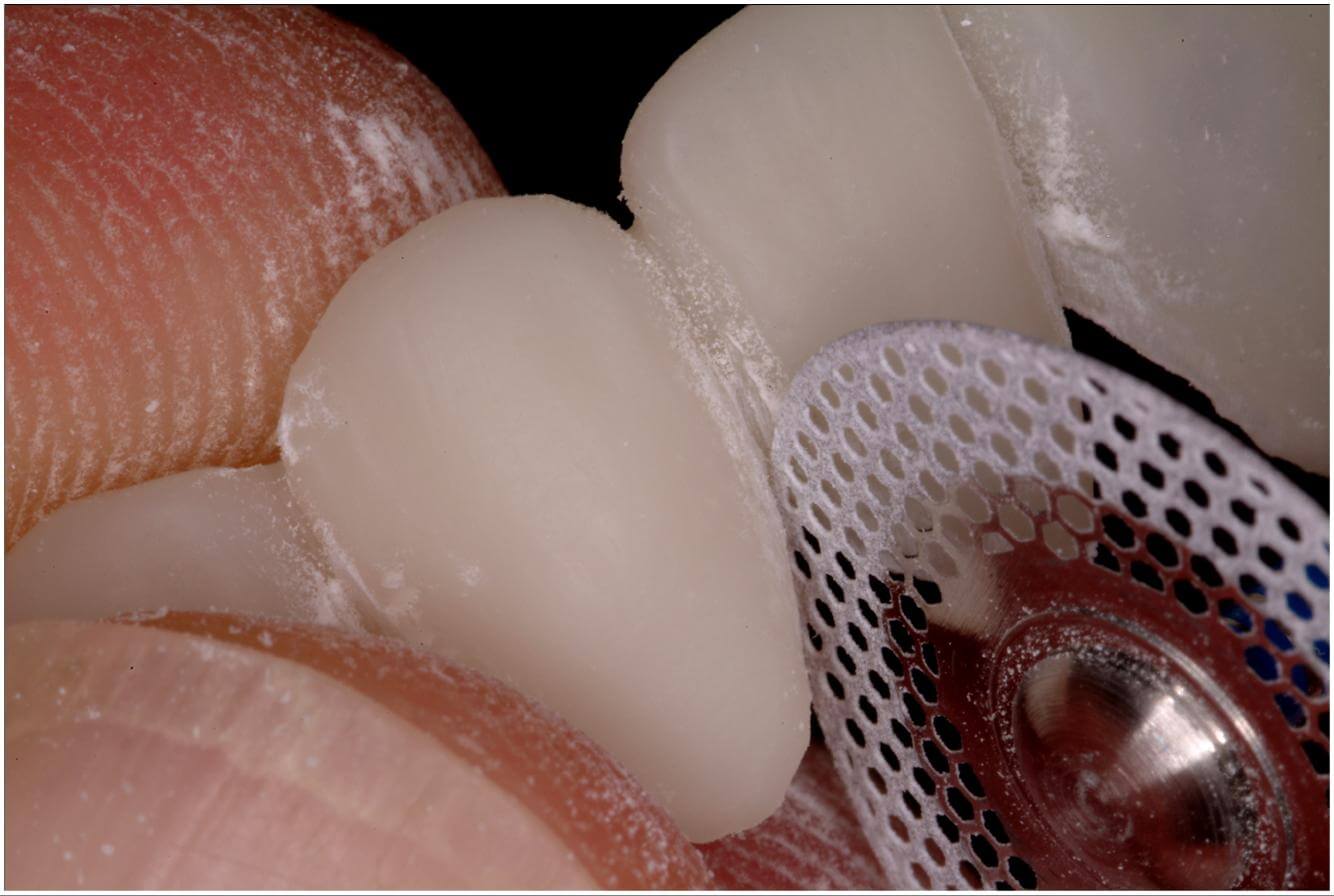
There are multiple components of an ideal tooth preparation, including distinct margins and sufficient tooth reduction. If you have to extend the material you are using into the gingival crevice, then you must ensure the intracrevicular tooth reduction is large enough to account for the cosmetic material that will inevitably recess into the tooth’s normal shape.
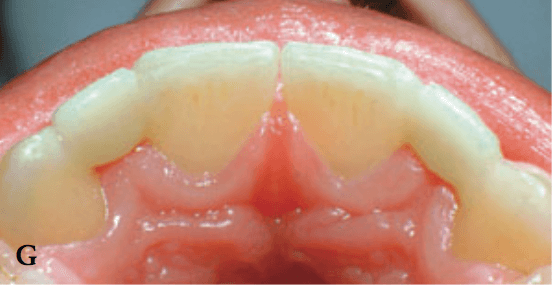
One thing that absolutely must be avoided is forcing cosmetic material out into the tissue. This can occur as a result of under reducing the cervical aspect of the tooth. The negative effects of this problem are plaque growth, decreasing the patient’s ability to adequately cleanse the area, and a crevice that appears flabby and retractable. You’ll see these problems happening because as the cervical bulge protrudes, it distends the crevicular epithelium and connective tissue.
Sometimes, you may put plenty of care and precision into your effort and still find that the tissue is injured during your tooth preparation. To avoid this, you can consistently follow these simple guidelines:
1. Don’t overextend the rotary instrumentation circumferentially.
2. Avoid permanently damaging surrounding tissue during retraction or while making impressions.
3. Create polished and excellently contoured margins, as well as a great fit, for the interim restoration.
4. Prevent retention of temporary cement in the gingival crevice.
5. Sustain control of intracrevicular plaque.
Follow these guidelines and you’ll be on your way to long-lasting results.
How do you go about enacting successful tooth preparation in your restorations? We’d love to hear from you!





Related Course
The Pankey Assistant’s Experience
DATE: June 12 2025 @ 12:00 pm - June 14 2025 @ 7:00 pmLocation: The Pankey Institute
CE HOURS: 17
Regular Tuition: $ 2050
Single Occupancy Room with Ensuite Bath (Per Night): $ 345
This “can’t miss” course will empower Dental Assistants to bring their skills to excellence! During this dynamic hands-on course, led by Pankey clinical team member, Sandra Caicedo, participants will learn…
Learn More>
About Author